In this article, I will be discussing the scope and powers of the Lasting Power of Attorney (LPA), the challenges doctors face in its issuance, and practical limitations in its implementation for donors. Suggestions on how social workers may help in mitigating the potential abuse of prospective donors and persons with diminished capacity (PDC) will also be presented.
Scope and powers of the LPA
The LPA is a legal document within the jurisdiction of the Mental Capacity Act 2008, administered by the Office of the Public Guardian (OPG). It allows a person who is at least 21 years of age (referred to as the "donor") to voluntarily appoint one or more persons (the "donee[s]"), to make decisions and act on his/her behalf if the donor loses mental capacity one day.
The donor may choose to grant his/her donee(s) decision-making powers over (a) personal welfare, which includes living arrangements, day-to-day care decisions, social activities, whom the donor may have contact with, etc; and (b) property and affairs such as accessing the donor's bank accounts to pay for his/her care, handling property, making investments, etc.
Donees may be non-professional individuals known to the donor who assume the role without remuneration. However, for the donee to be able to manage the donor's property and affairs, he/she must be at least 21 years old and must not be undischarged bankrupts.
Professional deputies or donees on the other hand can be individuals (eg, lawyers, nurses, social workers) or organisations that are paid for the service. To note, such individuals cannot be related to the donor by blood or marriage, while organisations are only allowed to manage the donor's property and affairs.
Challenges in the certification process
The process in the issuance of the LPA involves the following steps:
- The donor completes the LPA form online via OPG Online (OPGO), detailing the powers to be granted to the donee(s).
- The donee(s) accepts the appointment via OPGO.
-
The donor visits a certificate issuer (CI) to have the LPA certified. The CI witnesses the donor's signing of the LPA.
LPA CIs may be accredited medical practioners, qualified practising lawyers or psychiatrists. In the CI guide issued by the OPG, CIs are to ensure that (a) the donor understands the purpose of the LPA and scope of authority conferred under it; (b) no fraud or undue pressure is being used to induce the donor to create an LPA; and (c) there is nothing else that will prevent an LPA from being created.
Donors are not required to inform their family members when they apply for an LPA. With family relationships being complex, this non-requirement is understandable. However, a Straits Times report in 2014 revealed that about 6% of donors (approximately 400) made decisions for non-family members to be their donees.1 This is not to be dismissed for it presents the risk of abuse of donors, in particular for individuals who might imminently be losing their mental capacity, if their donees were to hold the ill intent of abuse.
When doctors who are CIs do not have the resources to inquire into the detailed psychosocial circumstances of the donors in their consult rooms, this risk is increased.
Circumstances suited for referrals
When CIs have reason to believe that more information is required to further safeguard the prospective donor during the certification process, they can refer donors to social workers to discuss the LPA application.
Cases would be suited for referral to social workers to inquire into the donor-donee relationship if one or more of the following conditions apply: (a) the donee is not an immediate family member, or a kin to the donor; (b) the donee is someone (including relatives) the donor has known or is close to for a relatively short period of time; (c) the donor knows little about the background of the proposed donee; and (d) the donor-donee relationship is conflicting, tense, abusive or disengaged.
Additional considerations include if donors (a) appear anxious but decline to share their concerns; (b) possess mental capacity that barely qualifies them to make an LPA application, putting them at greater risk of undue influence; and (c) have difficulty understanding the implications of their decision, despite attempts to help them.
With the donor's consent, CIs can refer the donor to social workers in writing or via a phone call, providing the following information:
- The reasons for the referral (ie, the CI's request that the donor meets a social worker to discuss the LPA application and its implications in greater depth).
-
Name, NRIC number, address and a phone contact of the donor.
Cases requiring a more detailed assessment may be referred to social workers at the following Protection Service Centre:
TRANS SAFE Centre (Bedok)
Community Legal Clinic
Blk 410 Bedok North Ave 2, #01-58
Singapore 460410
Tel: 6449 9088
Email: transsafe@trans.org.sg
With the donor's consent, social workers will meet the donors and their proposed donees (if applicable and with consent) to conduct a psychosocial assessment and provide a summary of their assessment in writing or via a phone call to the CI, who makes the final decision with regard to the LPA certification.
Challenges in exercising the LPA for PDCs
While the LPA serves to protect the welfare of PDCs, it has its limitations when exercised. The loss of capacity in one area could lead a donee to think that an LPA is now "active", leading to the risk of him/her taking up wide-ranging powers over the donor's finance, health and welfare matters. There is an additional risk that donees may have inadequate knowledge of the implementation of the LPA, or not know exactly when the donor loses capacity. This results in the exercising of the LPA being taken into effect too early or too late.2
As part of the "many helping hands" approach to community safeguarding of PDCs, doctors are encouraged to inquire with PDCs in private if they have donees and/or caregivers, and screen for signs of abuse when PDCs are presented in their consult room.
The Elder Abuse Suspicion Index (EASI) © shared here can serve as a screener to do this. It was developed to raise a doctor's suspicion about elder abuse to a level at which it might be reasonable to propose a referral for further evaluation by social services, adult protective services or equivalents.3
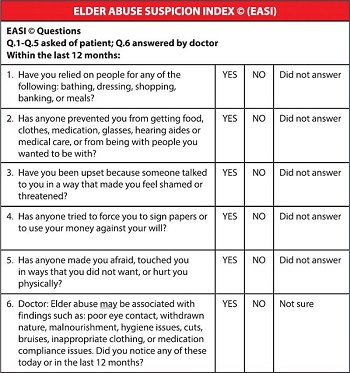
Reproduced with permission. EASI © tool developed by Mark J Yaffe (mark.yaffe@mcgill.ca), Christina Wolfson, Maxine Lithwick, Deborah Weiss. For detailed information, visit https://bit.ly/468mXqj.
While all six questions of the EASI © should be asked, a response of "yes" to one or more from questions 2 to 6 may establish concern. The EASI © was validated for family practitioners' use with cognitively intact seniors seen in ambulatory settings. The guiding questions may be applied for individuals with borderline diminished capacity in the community.
Should doctors identify signs of physical or psychology abuse and/or coercive control, which is often presented in subtle ways, they may phone the 24-hour National Anti-Violence and Sexual Harassment Helpline (NAVH) at 1800-777-0000. At the hospital or polyclinics, patients may be referred to medical social workers.
At NAVH, the case will be triaged and referred to the Domestic Violence Emergency Response Team at the Ministry of Social and Family Development (MSF), dedicated protection specialist centres or family service centres, depending on the risk level of abuse to the PDCs.
If abuse is established after conducting a risk assessment, safety planning will ensue at the social workers' office with follow-up monitoring. Cases will be escalated to the adult protective service at MSF if all efforts to engage and protracted efforts to help the PDC are blocked and/or in vain.
Doctors are encouraged to contribute to the safeguarding of PDCs, as the Vulnerable Adult Act accords protection to whistleblowers and professionals,4 when they act in good faith and with reasonable care.1
