Rostered routine testing (RRT) commenced among healthcare workers (HCW) in May 2021, and is still currently ongoing. In the initial two months, most centres seemed to have used the deep nasal swab technique for Polymerase Chain Reaction (PCR) tests. This survey, conducted in mid-August 2021, seeks to provide a snapshot of the perception of RRT by HCW. We are pleased that recent feedback indicates that most centres have changed to a self-administered Antigen Rapid Test (ART) instead. As we move towards an endemic state, we hope that the Ministry of Health (MOH) will continue to review this policy.
Introduction
In May 2021, there was a new cluster at Tan Tock Seng Hospital (TTSH), which led to the shutting down and diversion of services to other healthcare institutions to contain the outbreak. This brought about other stresses to the healthcare system.
To prevent another outbreak, MOH decided to implement RRT to all inpatient HCW, patients and visitors. This comprised the deep nasal swab for PCR, on a two-weekly basis for the vaccinated, or weekly if not vaccinated. More recently, the anterior nares swabs for the ART were included.
Similar RRT has been carried out in construction workers and maritime workers since June 2020.1,2 In speaking with Mr Bernard Menon, executive director of the Migrant Workers' Centre, to understand how migrant workers perceived RRT, we found out that the method of RRT was initially deep nasal swabs, but was later switched to the anterior nares swabs for ART soon after its introduction.
Anecdotally, the SMA Council received feedback on the medical side effects that RRT was causing, as well as challenges on the ground in its implementation. There was a diverse range of reactions. Some found the swabs fairly comfortable – just a little ticklish, even likened to digging one's nose. Yet others reported excruciating pain, akin to drilling into the back of the head.
Such varied responses might be attributable to various factors:
- Different swabbing techniques used,
- The experience of the swabber, and
- The underlying anatomy of the subject.
The methods and techniques of sample collection also vary significantly, including:
- Deep nasal (nasopharyngeal),
- Mid-turbinate,
- Anterior nares, and
- Back of throat.
The aim of the SMA survey was to understand HCW's perceptions toward RRT, and to find out if RRT caused significant side effects among the HCW.
Methodology
This was a one-time questionnaire-based survey, done via online survey platform SurveyMonkey. Brief consultations with the Chapters of Otorhinolaryngologists and Infectious Disease Physicians were held, in the compilation of questions for medical relevance.
The survey was launched on 11 August 2021 via email invitation to SMA Members and various modes of social media, and a second invitation via email and social media on 19 August 2021. The survey was closed after one month. Analysis of results were done on 11 September 2021.
Results
Response rates and characteristics of respondents
There were 2,202 unique respondents, of which 2,028 are undergoing RRT. There were 1,801 who completed the survey.
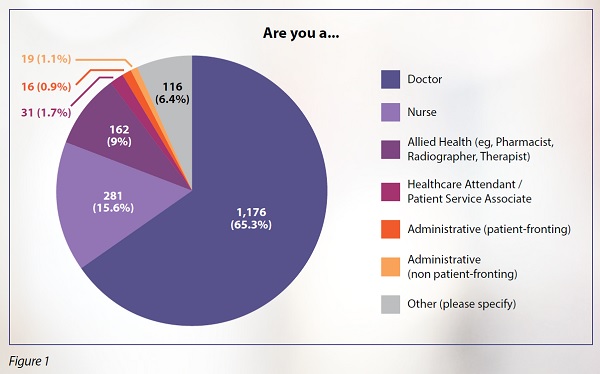
The majority of respondents were doctors at 1,176 (65.3%). 281 (15.6%) were nurses, 162 (9.0%) were allied health professionals, 31 (1.7%) were healthcare attendants/patient service associates, 16 (0.9%) were patient-fronting administrative staff, 19(1.1%) were non-patient fronting staff, and 116 (6.4%) identified as "Others"; giving a total of 1,801 complete responses (see Figure 1).
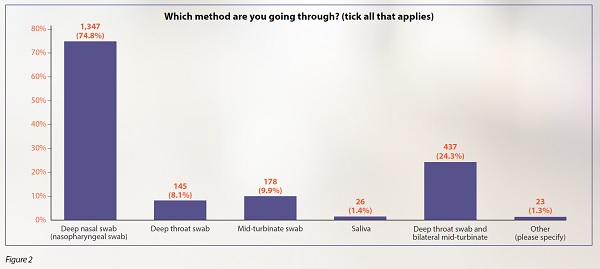
At the time of the survey, of those undergoing RRT, the majority (1,347 [74.8%]) were undergoing the deep nasal swab (nasopharyngeal swab), while the rest had a mix of different techniques (see Figure 2).
Adverse effects
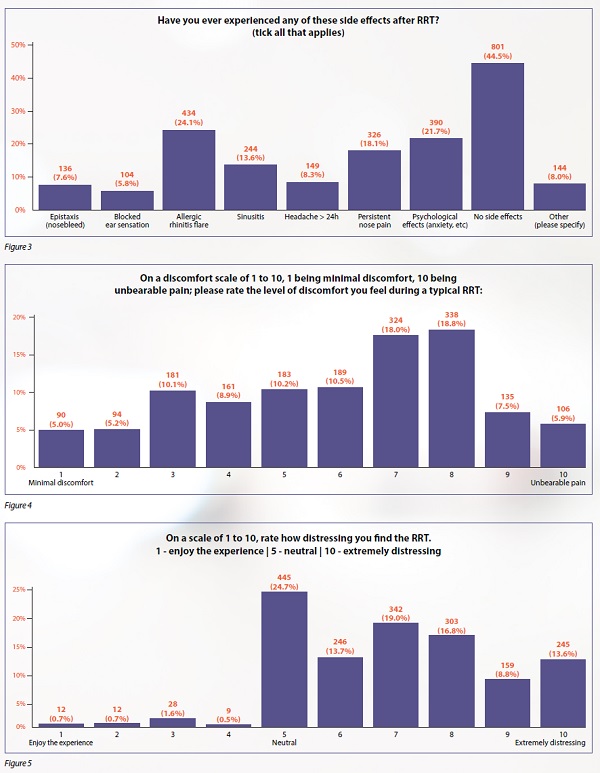
Among the respondents, 801 (44.5%) reported no side effects, while the remaining reported various side effects. For this question, respondents were able to select more than one side effect that applies as that may be a plausible scenario.
The most common side effect reported by the respondents was allergic rhinitis flare, with 434 (24.1%) affected, followed by psychological effects, with 390 (21.7%) affected. Other side effects such as nose bleeds, blocked ears, sinusitis, headaches and nose pains ranged from 5.8% to 18.1% (see Figure 3). 318 self-medicated for their reported side effects and a small minority of 37 respondents had to see a doctor.
Psychological impact
Discomfort scores from 1 to 10(1 being minimal discomfort and 10 being unbearable pain) seem to be fairly evenly distributed, with an average score of 6 out of 10.90 (5.0%) had minimal discomfort, 106 (5.9%) had unbearable pain, and more than 600 (36.8%) had scores from 7 to 8 (see Figure 4).
Regarding how distressing they found the RRT, 445 (24.7%) were neutral at 5 out of 10; 61 (3.4%) found it okay at less than 5, and 245 (13.6%) found it extremely distressing at 10 out of 10 (see Figure 5). 206 (11.4%) have considered changing jobs, to avoid the RRT.
Opinions on future RRT
1,458 (81.0%) prefer to have an alternative mode of RRT that is less invasive. 311(17.3%) were doing self-testing in addition to RRT.
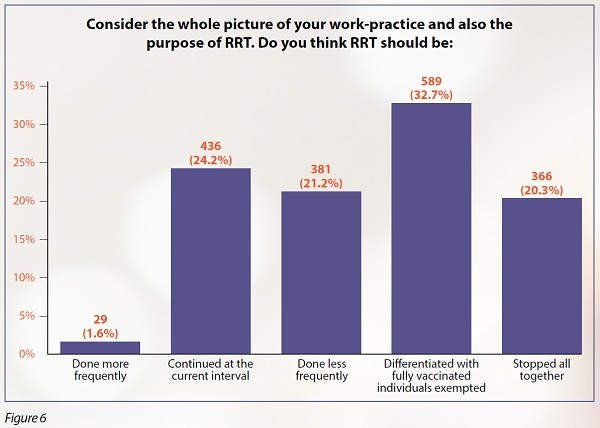
Opinions on how RRT should continue in the future were diverse. 29 (1.6%) felt that it should be done more frequently. 589 (32.7%) felt that it should be differentiated with fully vaccinated individuals exempted. The remaining were split quite evenly between the remaining three options: to continue at the current interval (once every two weeks), be done less frequently, or stopped altogether (see Figure 6).
Discussion
The majority of research has been focused on the basic science of the COVID-19 virus, its epidemiology, treatment and economic impact.There are a few studies on RRT in healthcare workers that study its pickup rate and its benefit in detecting early disease. This survey is the first study in Singapore, and possibly in the region, on the perception of healthcare workers regarding RRT.
The SMA is limited by funding and time, as we are a volunteer organisation. We advocate for doctors and for patients. In the ongoing COVID-19 fight, the SMA extends our representation to be a voice for all healthcare workers, especially in the planning of this simple survey.
We believe that this survey reflected these ground sentiments in the initial weeks of the RRT roll-out:
- There are a lot of resources being used for RRT: manpower, cost of materials and time.
- Our nurses are overworked, as they cover their usual clinical work, the additional precautions for COVID-19, keeping up to date with changing visiting policies and dealing with patient relatives, on top of swabbing duties.
- Routine work schedules are significantly disrupted.
- Some question the role of routinely swabbing to pick up well asymptomatic positives in the context of shifting towards an endemic COVID-19 Singapore.
Some of this feedback were informally provided to MOH and other authorities.
Ongoing questions to ask would include:
- Should RRT be done?
- If yes, what should be the appropriate,widely acceptable method:
- in acquiring the sample (eg, deep nasal swab, mid-turbinate, throat swab, saliva); and
- in running the tests: ART or PCR?
-
And what should the frequency of RRT be?
As demonstrated by the study, a significant portion of HCWs experience significant discomfort, adverse psycho-emotional effects and physical effects as a result of RRT. We believe that these contribute to chronic fatigue and burnout in this prolonged war against COVID-19. We hope to highlight the need to address these issues, and look forward to more studies to validate other modalities of screening which are less uncomfortable yet just as sensitive, and perhaps more cost-effective. As of mid-September, SMA received ground feedback that many healthcare institutions have shifted to superficial nares swabs for ART, some done by swabbers, some self-administered.
There are still logistics and cost challenges, due to record keeping and self-reporting, as some venues/centres may not accept self-swabs and demand a repeat swab. As Singapore moves towards an endemic state, we hope that RRT policies will be further defined in healthcare and other industries.